
Regenerative Spine Surgery · Naples & Fort Myers, FL
The 3R
Discectomy™
Remove. Replace. Regenerate.
A three-step regenerative protocol: remove the herniated disc through an incision
smaller than a quarter, replace the annular defect with Barricaid, and regenerate
with PRP biologic therapy — the most advanced disc surgery available in Southwest Florida.
"Remove what hurts. Replace what’s torn. Regenerate what’s damaged. That’s the goal — not just pain relief, but genuine disc healing."
Dr. G. Katsevman, MD · Fellowship-Trained, Barrow Neurological Institute18mm METRx tube
day of surgery
at 6 weeks post-op
for reherniation (Barricaid)
Who benefits
Are you a candidate for The 3R Discectomy™?
This procedure is designed for patients with a confirmed lumbar disc herniation causing leg pain, sciatica, numbness, or weakness who have not found lasting relief from conservative care.
Sciatica or Leg Pain
Sharp, shooting, or burning pain radiating from the lower back into the buttock, leg, or foot — often worse with sitting, coughing, or bending forward.
Confirmed Disc Herniation
MRI-confirmed herniated or extruded disc pressing on a nerve root. L4-5 and L5-S1 are the most common levels treated.
Failed Conservative Care
Physical therapy, medications, or injections have not provided lasting relief — or symptoms are severe enough to warrant surgical evaluation.
Reherniation Risk
Patients with a large annular defect face higher reherniation risk. When present and indicated, Barricaid seals the defect at the time of surgery.
The procedure
Remove. Replace. Regenerate.
Three steps. Each independently proven. Combined into one surgery — the most advanced approach to lumbar disc herniation available in Southwest Florida.
Remove — Minimally Invasive Tubular Discectomy
Traditional open discectomy requires cutting and retracting the large muscles of the back — causing significant tissue damage, more post-operative pain, and a longer recovery. Dr. Katsevman performs a fully minimally invasive discectomy through an 18mm METRx working channel, an incision smaller than a quarter.
The tube is dilated gently between muscle fibers rather than cutting through them, dramatically reducing trauma to surrounding tissue. A high-definition microscope gives Dr. Katsevman a magnified view of the nerve and disc fragment, which is then carefully removed to fully decompress the nerve root.
Patients walk the same day as surgery and go home the same day — no overnight stay. There are no activity restrictions at six weeks post-operatively.
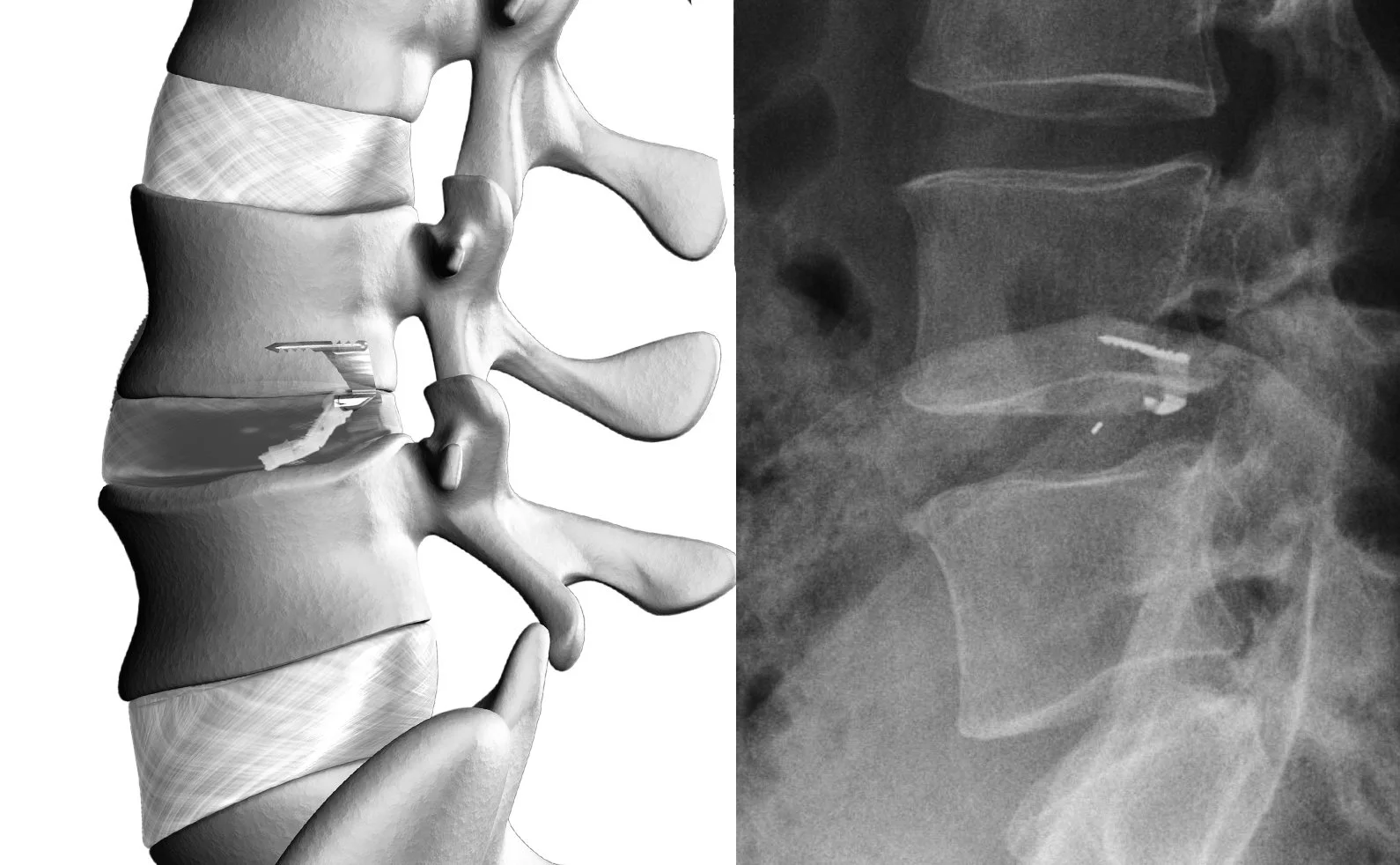
Replace — Seal the Annular Defect with Barricaid®
When a disc herniates, it tears through the outer disc wall — the annulus fibrosus. After the herniated fragment is removed, this tear (the annular defect) remains open. If the hole is larger than a standard pencil-top eraser (~6mm), the reherniation risk rises significantly — and 73% of all disc reoperations come from patients with these larger annular defects.
When the defect meets clinical criteria, Dr. Katsevman implants the Barricaid® Annular Closure Device — an FDA PMA-approved, bone-anchored woven implant that permanently seals the defect through the same incision, creating a barrier that prevents additional disc material from reherniating. Barricaid does not restrict motion and is anchored only to one vertebral body.
Clinical evidence across 8 distinct study populations — including 2 randomized controlled trials and over 70 peer-reviewed papers — shows an 81% reduction in reoperations for reherniation versus discectomy alone. Over 11,000 patients have been implanted worldwide, with follow-up as long as 10+ years. 92% of Barricaid patients return to work within 90 days.
Not every patient qualifies. Eligibility is evaluated before surgery and confirmed intraoperatively. When indicated, it is one of the most impactful additions available — the goal is to make your first surgery your last.
Regenerate — PRP Biologic Therapy
At the conclusion of surgery, Dr. Katsevman can apply Platelet-Rich Plasma (PRP) — a concentration of your body's own healing growth factors prepared from a small blood draw before surgery. A small sample of blood is drawn, spun in a centrifuge to concentrate the platelets and anti-inflammatory proteins, and then delivered precisely where healing is needed most — while you are already in the operating room. No extra procedure. No extra appointment.
PRP is delivered to three targeted locations:
Into the epidural space — injected around the spinal nerves to reduce inflammation, relieving leg pain and back pain. Clinical data shows a 36% reduction in back pain at 12 months, with relief building gradually and continuing to improve — unlike steroids, which decline after one month.
Into the disc space (intradiscal) — injected directly into the degenerated disc to restore hydration, support structural repair, and reduce degeneration. At 6–12 months, MRI confirms improved disc hydration, reduced inflammation, and preserved disc height — structural repair, not just pain masking. Disc reherniation rate with PRP: 1.33% vs. 8.75% without PRP.
Into the surgical incision — applied at the wound site to accelerate tissue healing and reduce post-operative complications.
Results from peer-reviewed clinical research (2023–2026): 73% of patients achieved clinically meaningful disability improvement at 1 year. 91% were satisfied and would recommend PRP at 1 year. 50% of patients reduced their pain medication use. Zero major adverse events across all major clinical trials.
PRP comes entirely from your own blood — no synthetic additives, no risk of allergic reaction or rejection. Because it is currently off-label for spine surgery, PRP is typically not covered by insurance and is offered as a patient-elected add-on.
How it compares
Traditional discectomy vs. The 3R Discectomy™
Standard / Traditional Discectomy
Large incision (1–3 inches)Requires cutting and retracting back muscles to access the disc.
Significant muscle disruptionRetraction causes damage, more pain, and a longer recovery.
Annular defect left openDisc wall tear remains unsealed — a pathway for reherniation stays open.
No biologic supportRecovery relies on baseline healing — no augmentation available.
Prolonged activity restrictionsOften involves weeks of limitations on bending, lifting, and movement.
Higher reherniation rateWithout annular closure, a significant percentage of patients re-herniate within 2 years.
The 3R Discectomy™ · Dr. Katsevman
Incision smaller than a quarter18mm METRx tube provides full surgical access through a tiny opening.
Muscle-sparing techniqueTube dilates between fibers — no cutting, less pain, faster return to activity.
Barricaid seals the defect (if indicated)Bone-anchored implant permanently closes the annular tear when present.
Optional PRP augmentationGrowth factors target the disc, nerve, and incision for accelerated healing.
Walk same day · home same dayNo activity restrictions at 6 weeks post-operatively.
Reduced reherniation riskBarricaid significantly lowers re-herniation likelihood and reoperation rates.
Common questions
What patients ask most
What is recovery like after the 3R Discectomy? +
Patients walk the same day as surgery and go home the same day — there is no overnight hospital stay. Most patients return to desk work within 1–2 weeks. At six weeks post-operatively, there are no activity restrictions. The minimally invasive tube approach causes far less muscle trauma than traditional open surgery, which is the primary driver of this rapid recovery.
Does everyone get the Barricaid device? +
No — Barricaid is indicated only for patients who meet specific clinical criteria, primarily those with a large annular defect confirmed during surgery. Dr. Katsevman evaluates eligibility before the procedure and makes the final determination intraoperatively. Not every herniation produces a qualifying defect, but when it does, Barricaid is one of the most impactful tools available to reduce the risk of reherniation.
Is PRP required, and does insurance cover it? +
PRP is completely optional — it is offered as a patient-elected add-on for those who want to pursue every available advantage in their recovery. Because PRP is currently off-label for spine surgery, it is typically not covered by insurance. The core discectomy is covered by most major insurance plans when medically indicated, and Barricaid coverage varies by insurer and plan. Our team will walk you through all cost details at your consultation.
Will insurance cover this procedure? +
The minimally invasive discectomy is covered by most major insurance plans when medically indicated. We work with all insurance plans — even if we are out of network, we can often utilize out-of-network benefits or pursue a GAP exception when surgery is part of your treatment plan. Our team will guide you through your specific options before any decisions are made.
Can I get a second opinion if I've already been told I need surgery? +
Absolutely — and Dr. Katsevman actively encourages it. A second opinion is one of the most important steps before any spine procedure. He offers in-person and telemedicine second-opinion consultations for patients across Florida and nationally. Bring your MRI images and prior records. Many patients find their surgical plan can be meaningfully refined after a second look.
What spine levels can be treated this way? +
The 3R Discectomy™ is primarily designed for lumbar (lower back) disc herniations — most commonly L4-5 and L5-S1, the levels responsible for the vast majority of sciatica cases. Dr. Katsevman also performs minimally invasive cervical (neck) disc surgery using a different approach. During your consultation he will review your imaging and determine the precise technique best suited to your anatomy and diagnosis.
"Remove what hurts, replace what’s torn, regenerate what’s damaged — that’s the 3R philosophy. Not just pain relief, but a genuine attempt at biological disc healing."
Gennadiy (Gene) A. Katsevman, MD
Neurosurgeon & Minimally Invasive Spine Surgeon
Fellowship-trained at Barrow Neurological Institute under Dr. Juan Uribe — a world pioneer in minimally invasive spine surgery
Neurosurgery residency, West Virginia University — Level 1 Trauma Center
30+ peer-reviewed publications in spine surgery and neurosurgery
Naples Top Doctor in Neurosurgery — 2024, 2025, and 2026
5-star Google rating · Healthgrades Choice Provider · WebMD Preferred Provider
U.S. News & World Report Patients' Top Choice
Offices in Naples and Fort Myers · Telemedicine available nationwide
Take the next step
Ready to discuss the 3R Discectomy™?
Schedule a consultation with Dr. Katsevman in Naples or Fort Myers — or via telemedicine — to review your imaging and find out if the 3R Discectomy™ is right for you.
6101 Pine Ridge Road #101
Naples, FL 34119
Fort Myers, FL 33919
Available nationwide

METRX Minimally Invasive Tubes
Barricaid Annular Closure Device

Platelet-Rich Plasma (PRP)